





January 14, 2019
 Cynthia S. Goldsmith and Yiting Zhang/CDC
Cynthia S. Goldsmith and Yiting Zhang/CDC
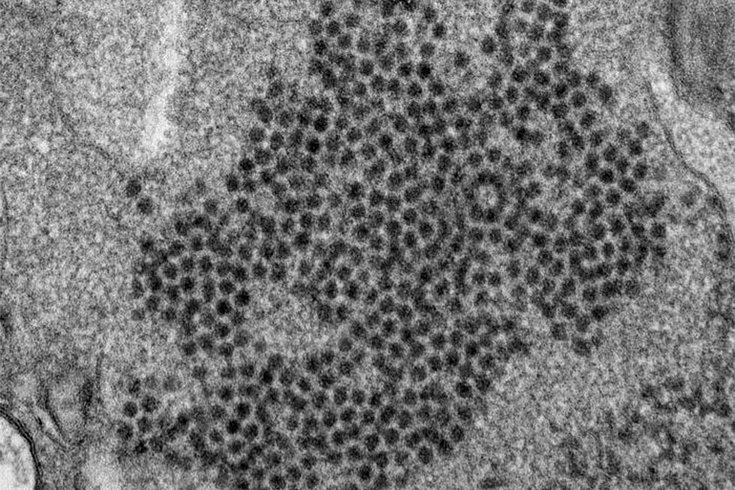
This photo from the CDC shows an electron micrograph of a thin section of enterovirus D68 (EV-D68), showing the numerous, spherical viral particles.
I experienced déjà vu when I took care of a child with acute flaccid myelitis in 2014, one of the first cases of its kind at the Children’s Hospital Los Angeles in many years.
I had taken care of polio patients in India in 1990s and also participated in the pulse polio campaign that led to the country successfully eradicating the devastating disease. But that was almost two decades back, and I had not seen polio or anything like polio since moving to the U.S. back in the late 1990s.
Now, the U.S. and several other developed countries are seeing outbreaks of this polio-like disease, stumping public health researchers on the reasons why.
Acute flaccid myelitis, or AFM, a descriptive term for the clinical manifestations, can be caused by polio or several other related viruses. The term acute stands for the fact that the onset is sudden; flaccid denotes that there is a loss of tone in the limbs that become weak; and myelitis indicates that the spinal cord is involved and abnormal. Acute flaccid myelitis falls under a broader category called acute flaccid paralysis – a term that encompasses several other conditions such as botulism besides acute flaccid myelitis.
According to the Centers for Disease Control and Prevention, there have been 519 confirmed cases of AFM in the U.S. since 2014. Most of them have involved young children.
The U.S. has been polio-free since 1979. The AFM cases in the U.S. since 2014 are polio-like but not due to poliovirus. The cause has been definitely established only in a handful of these recent cases with detection of coxsackievirus A16, enterovirus (EV)-A71, or EV-D68 in cerebrospinal fluid (CSF). These three viruses are types of enteroviruses just like poliovirus is. Enteroviruses are viruses that cause typically enter through the intestinal tract.
A majority of interventions tried in the initial stages of the disease to date have had no success.
Doctors have suspected that many of the recent AFM patients, in whom the spinal fluid did not identify a virus that caused AFM, may have been due to EV-D68. This is based on circumstantial evidence. At Children’s Hospital Los Angeles, where I practice and conduct research, my group has documented that EV-D68 was circulating in the respiratory fluid of children at a higher rate in 2016 when compared to 2015. This was associated with a higher rate of AFM in 2016 compared to 2015. According to the CDC, the spike in AFM cases in 2014 corresponded with a national outbreak of respiratory EV-D68. It is not known why only a handful of those who have the respiratory illness go on to develop AFM. Researchers hypothesize that genetic factors as well as unusual immune responses may be responsible.
The recent AFM cases have typically occurred in a cyclical pattern in late summer and early fall, and “skipped” a year, with more cases reported in 2014, 2016 and 2018 compared to 2015 and 2017.
Many children have symptoms suggestive of an upper respiratory tract viral infection and fever. This is followed by the most dramatic manifestation of weakness of arm or leg due to nervous system involvement. Either one or all four limbs may be affected. This is accompanied by a loss of tone and deep tendon reflexes. Sometimes, there may also be facial weakness or swallowing disturbances. In extreme cases, respiratory muscles are involved, leading to a need for artificial breathing support. The ability of patients to feel sensations is usually preserved, but pain is often prominent.
Once the disease is suspected, it is important that the child quickly undergo magnetic resonance imaging of the spine which typically shows changes involving the gray matter of the spinal cord. In cases with symptoms suggestive of cranial nerve involvement in the brain, such as facial weakness, brain imaging shows changes involving the gray matter of corresponding regions. Spinal fluid may show an increase in number of cells from what is otherwise found in normal children. Doctors may order nerve conduction studies and they show abnormal nerve impulses. The overall scenario with AMF is distinct and relatively easy to differentiate from diseases with some overlapping manifestations such as transverse myelitis and Guillain-Barré syndrome.
A majority of interventions tried in the initial stages of the disease to date have had no success. Drugs that work in several other neuroimmunological illnesses, such as intravenous immunoglobulins, and corticosteriods, have not been effective. Plasma exchange has been tried but has not shown benefit. Antiviral medications have not worked well either. Fluoxetine – an antidepressant – was noted to have in vitro antiviral property and efficacy against EV-D68, and tried by neurologists at several centers around the country in 2015 and 2016, including at my hospital. However, fellow researchers from centers around the country and I, led by Children’s Hospital Colorado, recently published our collective experience, noting that fluoxetine was not effective in improving outcomes.
The cornerstone of treatment in the initial phase is supportive care. Those with less severe manifestations at the outset are likely to do better in the long term than those with more severe initial presentation. Experimental surgical interventions with nerve grafting, after the acute phase is over, has shown some success in several patients.
The CDC has constituted a task force to investigate AFM. It is collaborating with the AFM Working Group, consisting of clinicians and researchers from around the country, in building a consensus to streamline treatment, in looking into and fostering research, and in leading advocacy efforts.![]()
Jay Desai, Clinical Associate Professor of Neurology, University of Southern California
This article is republished from The Conversation under a Creative Commons license. Read the original article.






